
A new patient group, called IamHH has been created to help both patients and health care professionals learn more about Kallmann syndrome and CHH. The group is registered as a not for profit patient charity group in the US and is applying for recognised patient group status with the National Organisation for Rare Disorders within the US.
The new IamHH group will have a new website and social media feeds. In order to help in the process of setting up the group a GoFundMe page has been set up for donations. Any help would be gratefully received and all funds will go to creating the website and generating resources to help patients.
A patient meeting has been organised by IamHH for Saturday 8th October 2022 at Boston College, hosted by Dr Andrew Dwyer.
A patient meeting is planned at Boston College, USA on 8th & 9th October 2022.
The meeting will be hosted by Dr Andrew Dwyer of Boston College. The meeting will be a good chance to meet fellow patients in a friendly, relaxed environment and to hear presentations from experienced KS medical experts.
There will a meal / drinks event for patients on the evening of the 8th October and a social event on the 9th October.
============================================================================
Recent medical paper on Kallmann syndrome / CHH
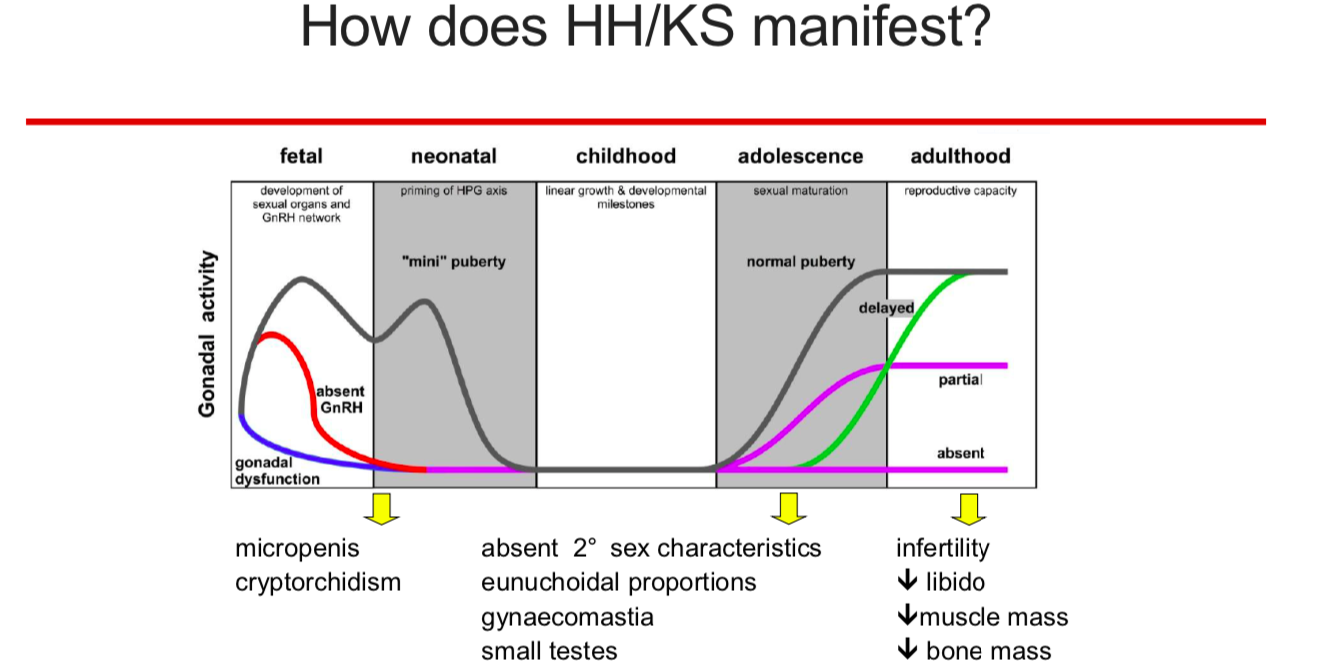
Kallmann syndrome / CHH are not easy to diagnose, especially if there is an absence of additional symptoms. In normal development there is a surge of reproductive hormones (LH / FSH / testosterone or oestrogen) that occurs soon after birth, between 1 and 6 months of age (a mini-puberty). This surge is more pronounced in males than females.
In Kallmann syndrome / CHH this surge is absent and a blood test to measure hormone levels soon after birth can help with an early diagnosis of Kallmann syndrome / CHH or help to eliminate it.
There is an on line patient meeting planned for Sat Jan 15th at 2pm EST / 6pm UK time. The meeting will be hosted by Dr Andrew Dwyer of Boston College, USA. The meeting will include a presentation by Dr Dwyer, a chance to ask questions and some updates on upcoming projects that could benefit patients.
Link to the meeting on Google.
There have been a couple of recent medical papers published on the use of the Kisspeptin test for diagnosing Kallmann syndrome / CHH. The idea is that the use of the protein Kisspeptin rather than the standard GnRH stimulation test can help doctors more easily distinguish between a case of Kallmann syndrome / CHH and a case of delayed puberty which would correct with or without treatment.
Earlier diagnosis and treatment of Kallmann syndrome / CHH, especially in teenagers can help with both the physical symptoms and probably more importantly, the psychological issues than can occur with the condition.
This post was made by a member of one of the Facebook KS groups. I thought it was worth sharing here as well:
2019 CHANGED ME-I was always an ordinary child like everyone else, I never had medical procedures that are more serious than tooth extraction and I never had serious diseases. I was healthy. However, one thing was wrong. I was 18 years old, and although 175 cm tall, I didn’t have any signs that puberty had started. I went to the endocrinologist for the first time in 2019, at the age of 18, and learned that unfortunately I am not one of the lucky late bloomers. I have a condition called Kallman Syndrome. By 2019 I was healthy, normal guy, and in 2019 I became a patient with a rare condition over night. I am starting to get informed about the condition and I am becoming more and more aware of my reality.Starting hCG+hMG therapy. That is how 2019 changed me.
2020 BROKE ME-I’m finishing high school, and I didn’t even get a chance to have a normal high school life because of KS and everything that comes with it. I lost a lot of friends that I never wanted to lose. I’ll never be a teenager. I missed the opportunity. Maybe there was a period in my life when I was 13-19, but it’s not enough to say that you were a teenager at one point in your life. I never was that and I will never be. I’m enrolling in faculty.
2021 OPENED MY EYES- hCG failed to help me produce testosterone… However, I began to realize that people do not have a bad opinion of me as I thought they did. I am beginning to learn that they respect and love me much more than I actually thought. I made good friendships with people from faculty and gained great respect from colleagues from faculty, as a testosterone deficient person . Every day I am more and more free from my traumas from my teenage days. I find out that I am as valuable as everyone else. Meanwhile, I am switching to testosterone. The last stage towards my complete transformation.Physical changes incoming, also mental and emotional ones that no one ever talks about,but they should. I may not have been a teenager, but improper development can be overcome with the right people around you. Having the body of a child at 20 is awful, but gaining respect from people around you with such body is not an impossible mission. A normal life is more than possible. EVEN WITHOUT TESTICLE ENLARGEMENT! A PERSON WITH KS CAN LIVE NORMAL LIFE!
2022-I’M COMING BACK-I’m coming back.Traumas from youth are a difficult enemy to overcome. And the worst are the ones that only you know how terrible and difficult they are to bear. Having KS is awful. KS patient is always in a dilemma what is worse, KS itself or the fact that no one will never trully understand you.But a normal life is possible. It is only necessary to go through these 4 phases. That is our development. That is how our development should be, that is what we are. We just need to find a way to live in accordance with that. I wish everyone a happy New Year, you may live with a rare condition, but you can live a normal life if you work hard enough. I wish you all the best!
A recent paper published by KS specialists working in Newcastle, UK, Italy and Singapore. A comprehensive overview of some of the current understanding of Kallmann syndrome / congenital hypogonadotropic hypogonadism (CHH).
Recent advances in understanding and managing Kallmann syndrome
There used to be a “wait and see” approach to delayed puberty but increasingly specialist endocrinologists have argued that recognising early “red flag” symptoms in patients with delayed puberty can help with earlier diagnosis & treatment which leads to better outcomes for the patient.
“Red flag” symptoms can include:
Anosmia / poor sense of smell
Hearing loss
Mirror movements of the hands
Missing a kidney
Undescended testicles – one or both
Fused fingers / toes
Cleft lip / palate
Absence of “mini-puberty” hormone surge in first six months after birth.
Not all symptoms will be present in all cases and the symptoms will depend on the genetic cause of each case of Kallmann syndrome / CHH. The genetic causes of Kallmann syndrome / CHH cover at least 30 different genes and their variants. Even these 30 genes cover barely 50% of cases which makes genetic testing for Kallmann syndrome / CHH difficult.
Testing with the Kisspeptin challenge test can help doctors distinguish between a case of delayed puberty rather than a case of Kallmann syndrome / hypogonadotropic hypogonadism. The Kisspeptin challenge test is thought to give a better indication of Kallmann syndrome / CHH than the standard GnRH challenge test.
Article from “The Mighty” website on social anxiety.
This says a lot about my early life as a teenager.
It is certainly not true for every person with Kallmann syndrome / CHH of course but I do remember the time as a teenager when I changed from a fairly normal kid to a very shy, socially distant teenager.
As my friends developed, both physically and socially, I felt left behind. Looking back this was totally my fault. After a while if you refuse social invitations or make up excuses not to go to events people will eventually stop asking.
I am certainly a shy individual and can find it difficult to socialise.
I am over 50 now but how I developed socially as a teenager and young adult has probably affected my whole life.
Kallmann syndrome / CHH can come in a range of severities and sometimes has additional symptoms so no two cases, even between siblings will be identical. However I do feel that puberty is an important step in the physical and emotional development of any person so any condition that prevents normal puberty from occurring must have an impact on a person. Just how severe that impact may be will depend on other circumstances such as age of diagnosis, availability of treatment and understanding about the condition.
Dr Andrew Dwyer of Boston College USA will be hosting an on line patient meeting on Saturday 12th June 2021 via Zoom.
The topic of this meeting will be “Psychological aspects of Kallmann syndrome / CHH including depression and anxiety.”
https://www.facebook.com/events/1636477733220159
Link to register for the meeting:
The psychological issues of having Kallmann syndrome are perhaps often overlooked in the treatment of Kallmann syndrome and CHH patients. Hormone replacement therapy can in a lot of cases help with the physical side of the condition but little attention is given to other aspects of the condition. Missing out on fundamental development stages such as puberty and adolescence can have a profound influence on a patient’s life.
On line patient meeting via Zoom hosted by Dr Andrew Dwyer of Boston College, USA.
It will be a chance to talk to fellow patients and to hear a presentation given by an experienced medical expert on Kallmann syndrome / CHH. There is no set topic for this meeting but Dr Dwyer will be giving a presentation to include fertility treatments and body image / intimacy issues.
The meeting will be followed by a focus group hosted by Dr Dwyer as part of his research into patient involvement in health treatment and information. A $20 Amazon gift voucher for participating in the group discussion is available.
Starting times:
4pm EST – Boston, USA,
9pm – UK, London,
8am (Sun 14th), – Sydney, Aus.
Link to register for the meeting and to receive the Zoom link:
I was diagnosed with Kallmann syndrome at the age of 23, I have now passed fifty. Over that time I had have the pleasure of meeting and talking to many fellow patients from different countries around the world.
Kallmann syndrome is a difficult condition to explain to other people. It is not even one condition, as the name suggests it contains a range of different symptoms, each which their own severity. I do not think any two cases are alike, with people having different additional symptoms such as deafness, scoliosis, cleft lip, fused fingers, missing kidney or they may show none of these additional symptoms. I myself am partially deaf.
The key detail is the lack of puberty and lack of reproductive ability. Even this varies from person to person, with some people having virtually no puberty at all, while some have partial / incomplete puberty.
Anosmia is an additional symptom found in Kallmann syndrome patients only but not in patients with the associated condition hypogonadotropic hypogonadism. My anosmia does not bother me too much but it does get noticed from time to time.
These are only a few of my personal views that have occurred to me.
Kallmann syndrome is an invisible condition. I do not look ill, I do not look like I need to take medication. In fact I do not even have to take my medication but being on medication does greatly improve my quality of life.
Kallmann syndrome is most certainly not the same as being a late bloomer or late developer. I never went through a normal puberty even when on treatment. I am infertile unless I take specialised gonadotropin medication and even that can take at least 2 years to work. Since I was late diagnosed and started treatment late I have an undersized / below average size penis and under sized testicles which have not grown since childhood.
I used to take testosterone as either an injection or gel. Currently I take a medication called hCG – human chorionic gonadotropin that allows me produce a low level of natural testosterone.
I was almost totally asexual throughout my teenage years and early 20’s. I tried to ignore that side of my life as best I could. I think having the condition has partly affected my ability to have both physical and emotional relationships but I made mistakes along the way that did not help either. I see myself as being bisexual now.
I think that is enough text for now. I do enjoy the chance to talk about and write about my condition to help raise awareness for others with the same condition. I think it helps me a lot. If you have got this far, thank you for reading.
There is a on line patient meeting via Zoom planned for Sat 7th November. The meeting will start at 11am EST / 4pm London time.
The meeting will be hosted by Dr Andrew Dwyer of Boston College, USA. It will be a general meeting with any topic covered and questions can be submitted in advance.
